
|
From the previous post found here I hope everyone understands more about cholesterol and why we need it. I am afraid that this next post requires a little high school chemistry but bear with me as I think you will find it of great benefit. Let's start with the high school chemistry. Anybody who has tried to clean a greasy pan with water has realized very quickly that fat and water don't mix. In order for the grease to "dissolve" in the water it needs soap. The same thing is true of cholesterol. The cholesterol in our bodies needs a special particle called a lipoprotein to carry it in our blood otherwise it will not dissolve properly. This particle contains proteins called apoproteins, phospholipids, cholesterol, cholesteryl esters, and triglyercides (fat). See the figure below. 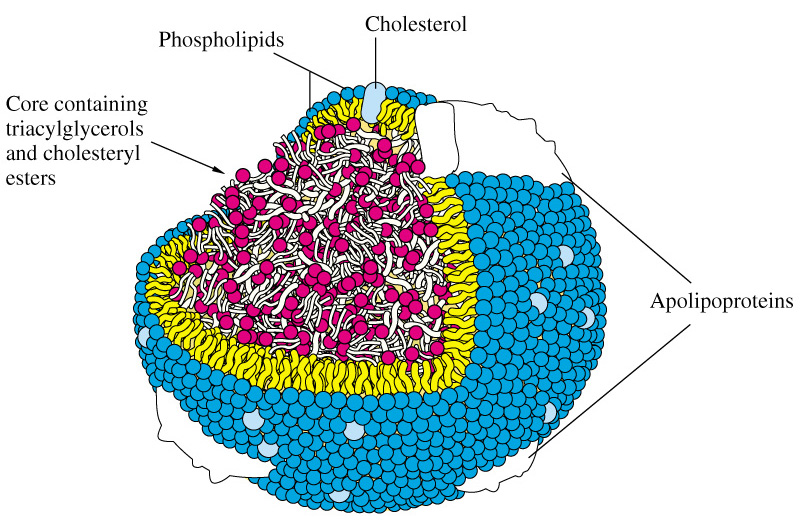 The apoproteins serve several functions including binding to cell receptors where the cargo needs to be dropped off. Apolipoproteins come in different forms. Two of the major forms are apoliprotein A-1 (apoA-1) and apolipoprotein B (apoB). The majority of apoB in our body is found on low-density lipoprotein. You might know this particle by the term "LDL" or the "bad" cholesterol. ApoA-1 is found on high-density lipoprotein otherwise known as "HDL" or "good" cholesterol. For every one particle of LDL there is one particle of apoB (specifically apoB100). The density of lipoproteins are defined by their lipid-protein ratio. In terms of lipoproteins there are 5 main classes or densities. These include chylomicrons and high (HDL), Intermediate (IDL), low (LDL), and very low-density lipoproteins (VLDL). HDL is the smallest and most dense followed by LDL, IDL, VLDL, and chylomicrons. Chlyomicrons, VLDL, and IDL have the most fat content and LDL has the most cholesterol. See the figure below. 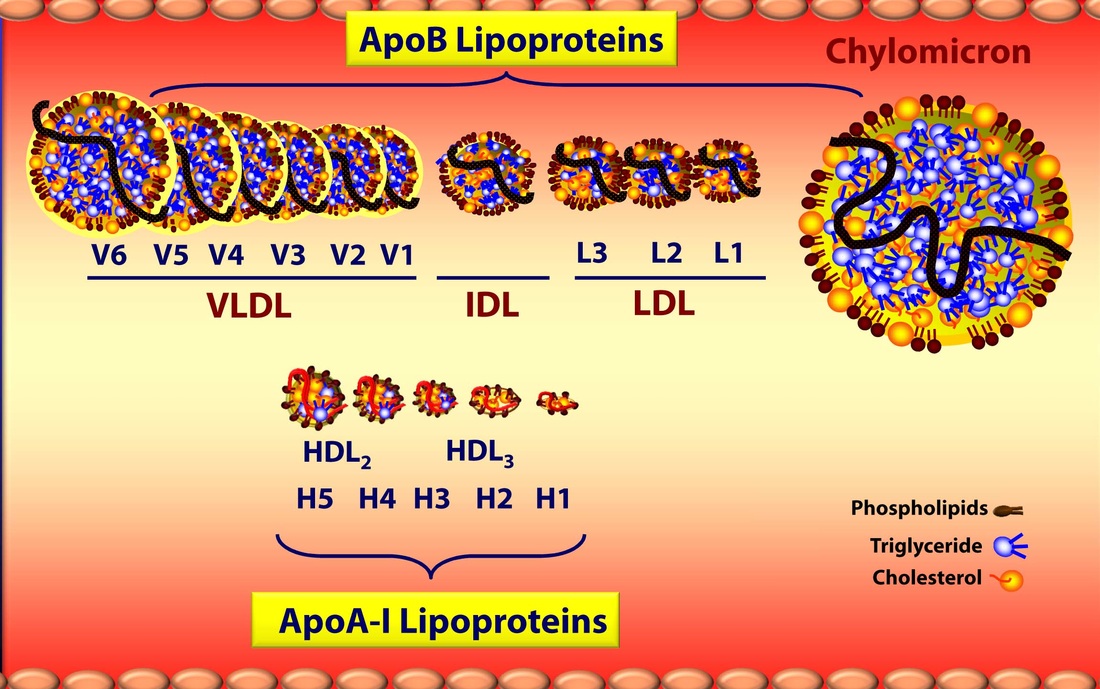 Interestingly the cholesterol concentration increases and triglyercide concentration decreases as the size of lipoproteins decrease.
The reason for this is that chylomicrons and VLDL come loaded with fatty acids from the gut and liver respectively. As they move throughout the body they release their fats to the muscle and adipocytes (fat cells) and shrink. As they do so they morph into IDL and then some eventually make it into LDL particles. As they shed fat they become more concentrated in cholesterol. Unfortunately, it is the LDL that can penetrate and deliver cholesterol to the arterial walls leading to atherosclerosis. It is also LDL that returns cholesterol back to the liver. The problem of the cholesterol dumping from LDL is the critical issue that we will discuss in the future. Stay tuned for part 3 in a few days. Also, I would like to acknowledge that I have gotten much of this information from Dr. Attia and his excellent blog. If you would like a personalized assessment of your cardiac risk factors and cholesterol numbers feel free to schedule a consultation. Of course, each individual case is different and the advice in this post should not substitute for getting a consultation with your doctor.
0 Comments
One of the common misconceptions out there is that cholesterol is "bad". The truth is that cholesterol is essential to life. Each of our cells is surrounded by a cell membrane that is composed of a "lipid bilayer". Cholesterol is a one of the key components of this membrane. Cholesterol also serves as a vital component in the production of vitamins and hormones including testosterone, estradiol, cortisol, and aldosterone. These hormones are essential to life. See the figure below for a visual representation of how cholesterol serves as a precursor for these key hormones. 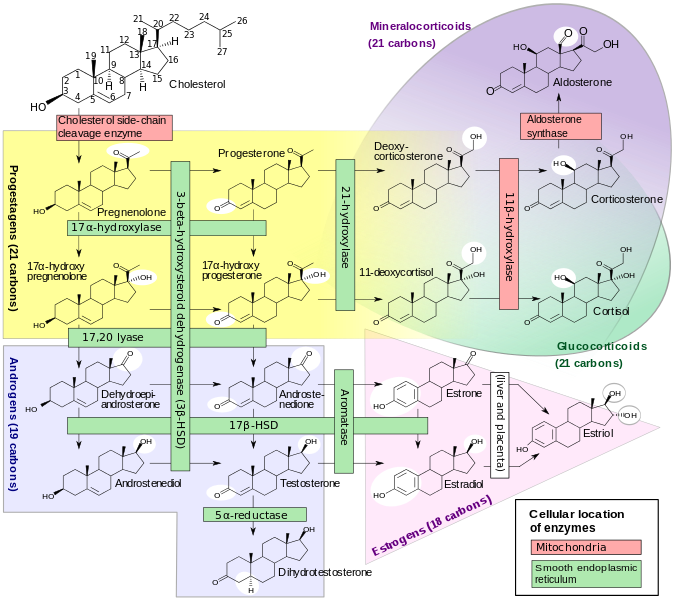 Because there is poor understanding about the critical role of cholesterol in our bodies we have been led to believe that there is "good" cholesterol and "bad" cholesterol. Nothing is farther from the truth. Cholesterol is good.
However, cholesterol can lead to "poor" outcomes when it gains access to the wrong places in our body like our arteries. From a clinical perspective this is especially pertinent when we are talking about coronary artery disease (CAD) which is by far and away the leading cause of death in this country. Cholesterol, I guess, is much like money. Money has been critical to the development of efficient and effective trade. Without it we would be bartering all day long for what we need. At the same time investment of money in the wrong areas can lead to unfavorable financial conditions. Likewise, when cholesterol gains entrance into our arteries it leads to an inflammatory cascade which can lead to narrowing and obstruction. This can eventually lead to heart attacks or strokes. So the next logical question is how can we determine if and when cholesterol will invade our arteries? Since CAD is the number #1 killer in America this question is pertinent to almost everyone. The problem lies in the fact that when you get your cholesterol measured we are actually measuring the total cholesterol amount in the blood. This doesn't necessarily tell us if and when these molecules will get into our arteries. And that is where I will leave off for now. Stay tuned for the next article in a few days. Also, I would like to acknowledge that I have gotten much of this information from Dr. Attia and his excellent blog. If you would like a personalized assessment of your cardiac risk factors and cholesterol numbers feel free to schedule a consultation. Of course, each individual case is different and the advice in this post should not substitute for getting a consultation with your doctor. |
Doctor/Telemed/Sick Visit $60

PREMIUM $45-60/MO
WEIGHT LOSS $60 HCG DIET $399 HORMONE VISIT $60 BLOOD WORK $60 LACERATION $150 STEM CELL $999 Testosterone Visit $69 Vitamin B12 $25 Archives
June 2022
Categories
All
|