
|
One of the most common patient issues that I see at my office is when someone comes in for nausea and/or vomiting. The reason for this is that nausea and vomiting is not only very annoying but also associated with some serious medical conditions. Consequently, there is some real anxiety around persistent vomiting.
So what are the top causes of vomiting and how do they differ by age group as taken from the online resource Uptodate? Neonates: Acid Reflux: Physiologic gastroesophageal reflux in newborns and infants is common, and is characterized by effortless regurgitation in an otherwise healthy infant (a "happy spitter"). This symptom may be described as vomiting by parents. The symptom gradually improves in most infants during the first year of life, and may be minimized by conservative antireflux measures. Food Intolerance: Intolerance to dietary proteins (most commonly milk protein) typically manifests as colitis, presenting with bloody stools. However, in some infants the dietary protein causes enteritis, with or without associated colitis, and affected infants may present with vomiting, diarrhea, and failure to thrive. Intestinal Obstruction: There are multiple causes of intestinal obstruction in neonates and young infants. Older Infants and children Gastroenteritis: Gastroenteritis usually is viral in etiology, occurring in clusters, sudden in onset, and quick to resolve. Bacterial causes may be associated with more prolonged and severe illness. Other Infections: Pharyngitis (particularly streptococcal pharyngitis) and urinary tract infections frequently present with nausea and/or vomiting. Adolescents In addition to the disorders affecting children listed above, some of the more common causes of nausea and vomiting in adolescents include gastroenteritis, appendicitis, inflammatory bowel disease (IBD), pregnancy, and toxic ingestions. The good news is that in my experience the majority of cases of nausea and vomiting resolve without serious ramifications. However, there are certainly times when seeing a doctor is necessary such as when there is significant abdominal discomfort, prolonged or vigorous vomiting, bloody vomiting, high fever, dehydration, or when someone is not improving. Of course, the advice in this post should not be substituted for the advice of your personal physician. If you have a need to be seen for this issue I can certainly help.
0 Comments
One of the most common recommendations out there is that we should floss daily to help reduce cavities and improve dental health.
There is only one problem. There is actually very weak evidence that flossing actually helps reduce cavities. According to the Associated Press: "The federal government has recommended flossing since 1979, first in a surgeon general's report and later in the Dietary Guidelines for Americans issued every five years. The guidelines must be based on scientific evidence, under the law. Last year, the Associated Press asked the departments of Health and Human Services and Agriculture for their evidence, and followed up with written requests under the Freedom of Information Act. When the federal government issued its latest dietary guidelines this year, the flossing recommendation had been removed, without notice. In a letter to the AP, the government acknowledged the effectiveness of flossing had never been researched, as required. The AP looked at the most rigorous research conducted over the past decade, focusing on 25 studies that generally compared the use of a toothbrush with the combination of toothbrushes and floss. The findings? The evidence for flossing is "weak, very unreliable," of "very low" quality, and carries "a moderate to large potential for bias." "The majority of available studies fail to demonstrate that flossing is generally effective in plaque removal," said one review conducted last year. Another 2015 review cites "inconsistent/weak evidence" for flossing and a "lack of efficacy." I have never been a big fan of flossing but I am a big fan of looking at the data. While it will probably not do damage for most people to floss and there may be some benefit I think there is a lot of undo fear out there that if you don't floss it will definitely lead to cavities. The current level evidence seems to say that this is not the case. More rigorous studies are definitely needed to test the efficacy of flossing. Ultimately, whether you decide to floss or not is up to you. Of course, I would recommend consulting with your dentist before making any changes to your dental hygiene regimen. " You may have seen a lot of headlines recently about drug resistant super lice that is now spreading throughout the United States. A whopping 42 out of 48 states tested are overrun by this so-called super lice, according to a study published in the Journal of Medical Entomology. The map of the United States below shows resistant lice in 100% of Texas samples. 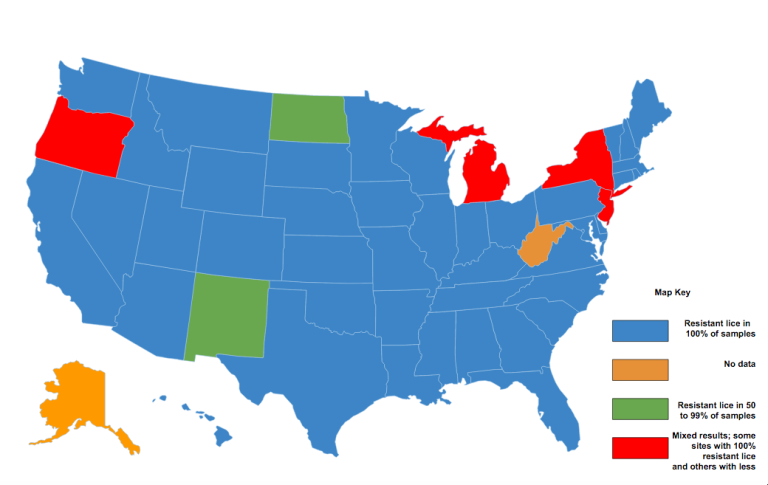 The problem is that the so-called "super lice" has mutated such that it is now resistant to most over the counter treatments.
The current recommendations from some health care professionals is that it is still reasonable to give over the counter treatments a couple tries separated by a week before needing to see a Doctor. The good news is that there are still prescription options that are effective even when the over the counter options fail. If you need to see someone about lice I am happy to help or you can see your own PCP. The following general information about Lice is taken from an online physician resource. HEAD LICE SYMPTOMS — Most people with head lice do not have any symptoms. Some people feel itching or skin irritation of the scalp, neck, and ears. This is caused by a reaction to lice saliva, which the lice inject into the skin during feeding. HEAD LICE DIAGNOSIS — Head lice are diagnosed by examination of the scalp and hair. Special "nit combs" can be used to assist with the diagnosis. ●Before using the fine-toothed comb, use a regular brush or comb to remove tangles. This can be done while the hair is wet or dry. If the hair is wet, apply hair conditioner to make the hair easier to comb. ●Place the fine-toothed comb at the top of the head, touching the scalp. Pull the comb through the hair from roots to ends. After each stroke, carefully examine the comb for lice or eggs. ●Comb the entire head at least twice Finding eggs (nits) without lice does not necessarily mean that there is an active infestation; nits can be found for months after lice are treated. Because lice lay eggs at the base of the hair shaft, the identification of nits within ¼ inch of the scalp suggests (but does not confirm) an active infestation [3]. Lice can be more difficult to see than nits since they can move and hide from view. A doctor or nurse can examine the head under a special lamp, which causes nits to glow a pale blue color. If you are unsure whether your child has lice, make an appointment for your child to be examined before you start treatment. Finding head lice can be upsetting to children and parents, but it is important to keep the following in mind: ●Head lice are not a sign of being dirty or sick ●You can get rid of head lice with proper treatment ●There are no serious or long-term health problems associated with head lice HEAD LICE TREATMENT — There are several options for getting rid of head lice, including creams and liquids, combing, and oral medicine (pills). It is important to follow directions carefully to be sure that the treatment works. If you are sure that your child (over age two years) has head lice, you can use a nonprescription lice treatment. Examine family members and close contacts at the same time and treat them if needed. If your child is under age two years, contact the child's doctor or nurse for treatment advice. Insecticides — A topical insecticide (pediculicide) is a substance, usually a lotion or gel, that is applied to the scalp to kill lice. Available insecticides include: ●Permethrin (Nix, Rid) ●Pyrethrin (A-200, Pronto, Tisit) ●Malathion (Ovide, prescription required in the United States) ●Benzyl alcohol (Ulesfia, prescription required) ●Spinosad (Natroba, prescription required) ●Topical ivermectin (Sklice, prescription required) Follow the manufacturer's instructions for applying the insecticide carefully. Typically, you wash the hair with shampoo, rinse it, and towel-dry it. Apply the insecticide cream or gel liberally to the scalp and leave on for 10 minutes before rinsing with water. Malathion (Ovide) should be left on the scalp for 8 to 12 hours or overnight. Malathion has a bad smell, which can be hard for some people to tolerate. Malathion is also flammable and should never be applied in close proximity to fire or electric heat sources (such as a lit cigarette, curling iron, or hair dryer). A second treatment is needed with permethrin, pyrethrin, and benzyl alcohol 7 to 10 days after the first treatment. This is because some lice are able to survive the first treatment. A single application of malathion often is sufficient. However, malathion should be reapplied if live lice are seen seven to nine days after treatment. Treatment with spinosad should be repeated if live lice remain after seven days. Topical ivermectin is given as a single treatment; patients should consult with a healthcare provider before repeating treatment. Wet-combing — Wet-combing is a way to remove lice from the hair with careful and repeated combing. It is a good option for treating very young children or if you want to avoid using insecticides. However, wet-combing is time consuming and must be repeated multiple times over a period of a few weeks. Wet the hair and add a lubricant, such as hair conditioner or cream rinse, vinegar, or olive oil. See above for a description of how to wet-comb. The combing session should take 15 to 30 minutes, depending how long and thick the hair is. Comb every three to four days for two weeks AFTER you find any large, adult lice. Oral medicines — A medicine taken by mouth called ivermectin might be prescribed for people whose lice are resistant to topical insecticide treatment. Other treatments — Studies have examined lotions and other materials (olive oil, butter, mayonnaise, petroleum jelly [Vaseline]) that are applied to the head, and then allowed to dry, with the goal of suffocating lice. However, lice are difficult to suffocate; wet-combing probably works as well and is less messy. Lice treatments that use gasoline or kerosine are toxic and can lead to serious injury and should not be used. We do not recommend any of these treatments. PREVENTING HEAD LICE SPREAD — Adults and children who live with a person diagnosed with lice should be examined for lice and treated if needed. Anyone who sleeps in the same bed should be treated for lice, even if no lice or eggs are found. School policies differ about who at a school, if anyone, needs to be informed when a child has lice. A confidential call or visit with the school nurse is a good place to start. Most experts believe that children with head lice do not need to be removed from school. Clothing, bedding, and towels used within 48 hours before treatment should be washed in hot water and dried in an electric dryer on the hot setting. Dry cleaning is also effective. You can use a vacuum to clean furniture, carpet, and car seats. Items that cannot be washed or vacuumed can be sealed inside a plastic bag for two weeks. Items that the person used more than two days before treatment are not likely to be infested because head lice cannot survive off the body for more than 48 hours. You do not need to have your home sprayed for lice. |
Doctor/Telemed/Sick Visit $60

PREMIUM $45-60/MO
WEIGHT LOSS $60 HCG DIET $399 HORMONE VISIT $60 BLOOD WORK $60 LACERATION $150 STEM CELL $999 Testosterone Visit $69 Vitamin B12 $25 Archives
June 2022
Categories
All
|